A male in his 80s presented with gross hematuria. On CT of the abdomen, there was a plaque-like thickening of the bladder wall measuring 7 x 6.5 x 2 cm with “fat stranding”. On cystoscopy, no distinct bladder mass was identified and a biopsy was performed.
Previous
Next
Quiz
1. What is the correct diagnosis?
a. Scar
b. Vasculitis
c. Post-transurethral resection granuloma
d. Amyloidosis
e. Normal bladder
2. In primary involvement of the urinary bladder, what is the most common protein involved?
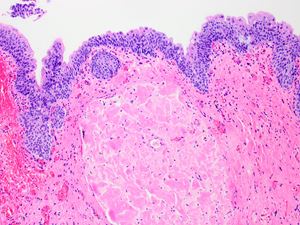
Bladder amyloidosis is a rare entity that has been described in case reports and case series. It has been found to coexist with urothelial carcinoma in some cases (Sirohi et al.). It can be either primary (localized) or secondary (due to systemic involvement). Primary localized amyloidosis is more common in older adults (mean age 55) with a slight male predominance. The presentation includes gross hematuria and irritative or obstructive voiding symptoms. The cystoscopic appearance is variable and can include edematous/hemorrhagic areas, yellow plaques, bladder wall thickening, and polypoid masses mimicking malignancy. Primary amyloidosis is most often composed of immunoglobin light chains, although a recent case series reported transthyretin to also be common, and is thought to be due to chronic cystitis and inflammation. Secondary amyloidosis is less common; clinical workup is usually recommended to exclude a systemic involvement.
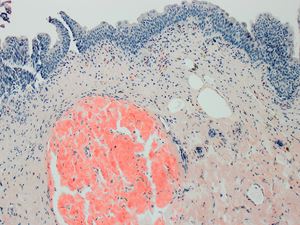
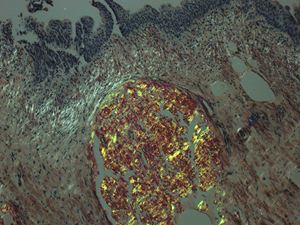
Amyloidosis represents deposition of protein in a β-pleated sheet conformation as insoluble eosinophilic extracellular material. It is most common in the lamina propria of the bladder, but it may also be perivascular, as illustrated in this case. A perivascular deposition is more common in the secondary amyloidosis. The deposits are salmon-pink/orange on Congo red stain and demonstrate an apple-green birefringence when polarized. This staining pattern confirms the diagnosis of amyloidosis, but does not specify the type of amyloidogenic protein; this can be done by immunohistochemistry or laser microdissection followed by liquid chromatography/mass spectrometry. Treatment for primary bladder amyloidosis involves transurethral resection as the treatment of choice. Recurrence is common and occurs in about 50% of patients.
Al-Obaidy KI, Grignon, DJ. Primary Amyloidosis of the Genitourinary Tract. Arch Pathol Lab Med. Published online May 8, 2020. doi: https://doi.org/10.5858/arpa.2020-0102-RA
Wilkinson M, Fanning DM, Flood H. Primary bladder amyloidosis. BMJ Case Rep. 2011 Jul bcr0520114211.
Javed A, Canales BK, MacLennan GT. Bladder amyloidosis. J. Urol. 2010 Jun; 183(6):2388-9.
Sirohi D, Gandhi J, Amin MB, Luthringer DJ. Amyloidosis of the bladder and association with urothelial carcinoma: report of 29 cases. Hum. Pathol. 2019 Nov 1; 93:48-53.